Alzheimer's Specialized Teams in the Grand Est region: A successful organization undergoing change
Regards No. 65 - September 2025
This study was conducted at the request of and with funding from the Grand Est Regional Health Agency
Authors: François Richou (Manager, GovHe); Véra Comolli (Senior Consultant, GovHe); Coralie Dumoulin, PhD (Senior Consultant, GovHe)
Alzheimer's Specialized Teams in the Grand Est region: A successful organization undergoing change
This article examines the role of specialized Alzheimer’s teams (ESA) in the care of people with neurodegenerative diseases in the Grand Est region. In the first section, we outline the context, the issues at hand, and the methodology used to conduct this assessment; in the second, we present the results and offer recommendations to improve the territorial coverage of the ALTs, taking into account the resources available to them and the environment in which the teams operate (available staff, user profiles, presence of caregivers, partnerships).
Through a detailed analysis, including surveys using scientifically validated questionnaires, focus groups, and individual interviews, the study highlights the successes and challenges of implementing ESAs in their regions. The results demonstrate the importance of better coordination between ESAs and their partners, the need to select user profiles suited to the services offered by ESA professionals, the need to enhance the appeal of the professions within these teams, and the necessity of adapting ESA specifications in light of changes in the profiles of the users they serve. This quantitative and qualitative study, supported by mapping data, will contribute to stakeholders’ efforts to adapt their local support strategies to the shift toward home-based care and inform ESA professionals in their ability to provide more integrated care for users and their caregivers. More broadly, this study offers potential solutions to decision-makers in light of current work on the national strategy for neurodegenerative diseases, the reform of home healthcare services (SSIAD), and the role of ESA in streamlining and improving the quality of the user care pathway.
Part 1: Background, Research Questions, Methodology
The ESA program stems from Measure 6 of the 2008–2012 Alzheimer’s Plan, and the circular defining the terms of reference is dated March 23, 2011. Attached to a home care service (SSIAD) with a minimum of 60 beds (or to a specialized home care service for people with dementia, SPASAD), ESAs aim to support people with Alzheimer’s disease (or other related conditions) living at home who have been diagnosed with mild to moderate-stage disease[1].
The care program consists of 12 to 15 sessions spread over a three-month period, with the option to renew after one year. Care provided by a personal care assistant (ESA), prescribed by a doctor and covered by health insurance, has several objectives. The teams strive to maintain users’ independence by stimulating their remaining abilities and mitigating behavioral issues. Additionally, they seek to improve the relationship between the person receiving care and the caregiver by relieving the latter of their burden and offering them respite while the ESA professionals care for the user.
The establishment of these ESA teams plays a significant role in promoting community-based care in the Grand Est region by providing specialized expertise, facilitating coordination with other healthcare professionals, delaying institutionalization, and supporting family caregivers. These teams thus offer personalized care tailored to the specific needs of service users.
Objective: To conduct an assessment of the 40 ESA
As part of the shift toward home-based care and with the aim of strengthening efforts to prevent the loss of independence, the Grand Est Regional Health Agency (ARS) commissioned a detailed assessment of the forty ESA facilities located in its region, focusing on two areas:
- At the regional level, by mapping out the ESAs, analyzing their human resources and caseloads, and then developing a classification system for the ESAs
- With regard to the ESAs themselves, by conducting an analysis of their operations in light of this typology.
This study made it possible to:
- To document the integration of ESAs into the care pathway for older adults with neurodegenerative diseases by gathering objective information on their effectiveness and impact
- Gain a better understanding of users’ support needs and highlight the impact of caregivers’ presence on compliance with the specifications;
- Assess whether organizations meet the ESA’s specifications.
Methodology: A 360-degree approach involving all stakeholders
A comprehensive, 360-degree approach was chosen to assess the current state of ESA in the Grand Est region.
First, we created comprehensive maps of ESA coverage, which allowed us to identify areas without coverage and compare their locations with the services available in the region. We categorized the ESAs based on their compliance with the specifications, taking into account full-time equivalents (FTEs) and the active caseload, in order to better identify areas requiring adjustment. This information was collected through an initial questionnaire sent to the ESAs (to which all organizations responded).
Next, we distributed an online questionnaire to participants to assess their quality of life using the ADR-QL scale[2], which allowed us to gather the perceptions and experiences of 250 respondents. This choice of tool facilitated the collection of reliable and representative data, which is essential for better understanding the direct impact of ESA interventions on the daily lives of people with Alzheimer’s disease. Caregivers, for their part, were invited to assess their own burden via a second online questionnaire using the ZARIT[3] scale. With 300 respondents, this assessment allowed us to precisely analyze the perceived burden and identify areas for improvement in support services, whether provided by ESAs or their partners.
The qualitative component of the evaluation, conducted with the ESAs, centered on focus groups involving more than 60 participants, supplemented by semi-structured interviews. This combination provided an in-depth understanding of the teams’ practices, challenges, and perspectives, while highlighting their expertise and on-the-ground experiences.
Next, the upstream and downstream partners of the ESAs were also involved through a focus group. This collaboration made it possible to develop a comprehensive overview of the ecosystem surrounding the ESAs and to identify areas for coordination and synergy to strengthen care pathways.
Finally, we also conducted a benchmarking study of seven ESAs in six other regions to compare practices and identify innovative approaches or areas for improvement. This comparative analysis enriched our assessment by providing a broader perspective on performance and regional adaptations, allowing us to compare the ESAs in the Grand Est region with those in other regions.
Part 2: Key Findings and Recommendations
A. The Grand Est region is currently almost entirely covered by the ESA, with a few areas still without coverage.
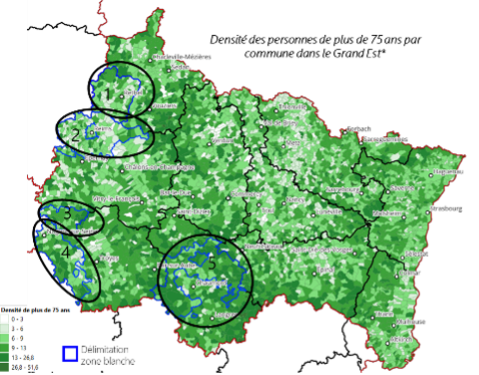
Five areas in the Grand Est region are not covered by ESAs (Map No. 1). These uncovered areas also exhibit significant variation in the proportion of residents aged 75 and older (Map No. 2) and varying densities of general practitioners, who are the primary prescribers of care (Map No. 3)
The coverage areas of the ESAs

Map No. 1
Card No. 2
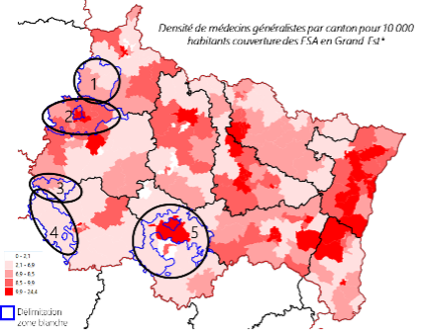
Card No. 3
Recommendation: Given the elderly population and the presence of general practitioners in the five identified underserved areas, establishing new ESAs or expanding the coverage areas of existing ESAs in these regions could help ensure comprehensive coverage throughout the region.
B. There are three distinct groups of ESAs: ranging from those most compliant with the ESA specifications to those furthest from them, based on the active caseload and FTE
Based on the questionnaires completed by ESA professionals, various data were collected. This data pertained to: operations (active caseload, waiting list, waiting times between the initial request and the start of care), human resources (distribution of full-time equivalents within the ESA and job profiles), the ESA’s service area (average distance traveled to reach users’ homes), users and caregivers (proportion of users over 90 years old, proportion of users with an MMSE score below 10, proportion of users with a caregiver), and partners involved throughout the care process (before, during, and after).
ESA Specifications
One ESA corresponds to 10 installed seats and a theoretical annual caseload of 120 users. The team consists of the following professionals:
- Nurse Coordinator (IDEC) responsible for partnerships, baseline assessments, and the coordination and monitoring of interventions (0.25 FTE);
- Occupational therapist and/or psychomotor therapist responsible for assessing the patient’s abilities, conducting rehabilitation and support sessions, and preparing a report for the attending physician (1 FTE);
- Geriatric care assistants (GCA) who provide some of the rehabilitation and support care based on the assessment and goals set by the occupational therapist and/or the psychomotor therapist (1.5 FTE).
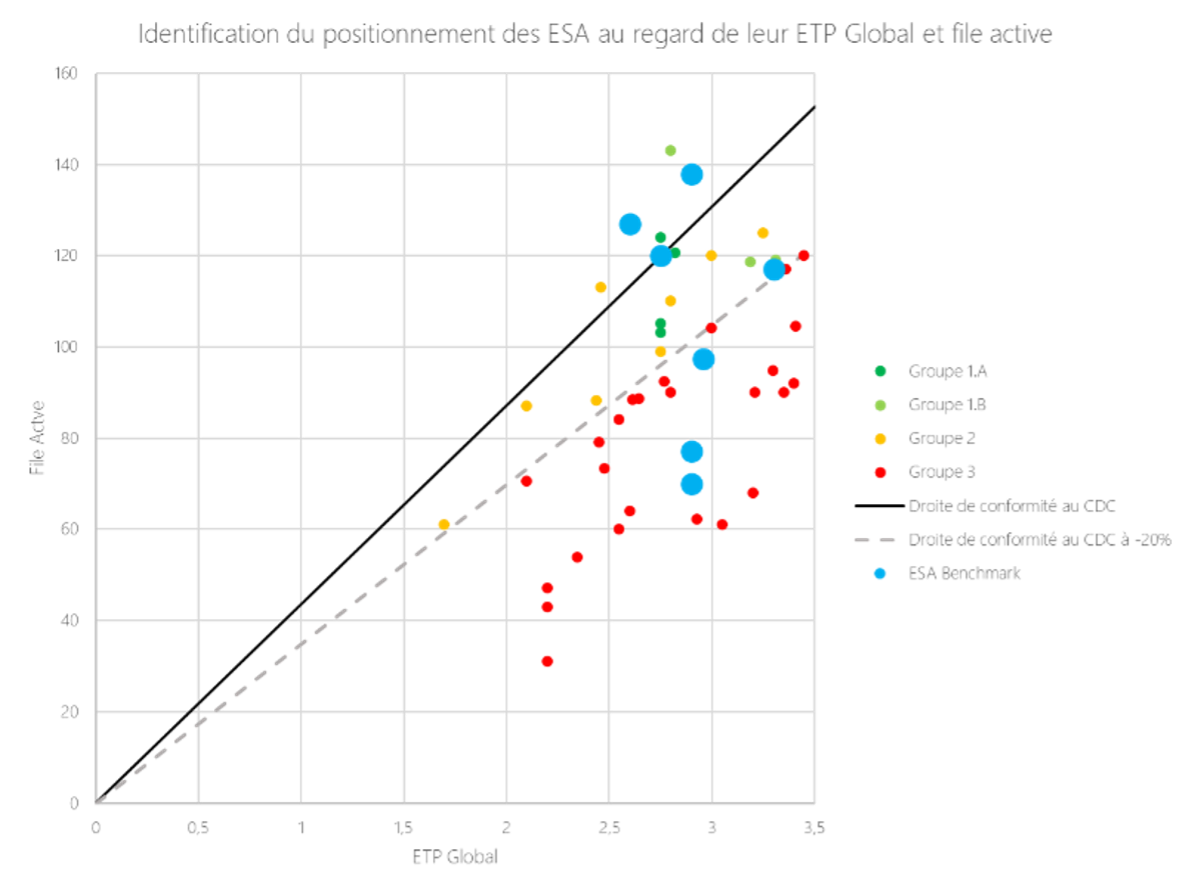
Analysis: The graph below presents the profile of each of the forty ESAs in the Grand Est region, represented by their active caseload and the number of FTEs in their workforce for the year 2023. The solid line represents “compliance with ESA specifications[4] ” (groups 1a and 1b[5]). The dotted line corresponds to “compliance with the ESA specifications at -20% in active caseload and/or FTE” (Group 2). Group 3 comprises the ESAs that are far from meeting the ESA specifications regarding active caseload and/or FTE criteria. The blue dots indicate the positioning of the seven ESAs from the six other regions. Regarding the active caseload and FTE criteria, we can draw two main conclusions. The first is that few ESAs comply with the specifications, which can be partly explained by the fact that these specifications date from 2012, with updates already underway as part of the national strategy for neurodegenerative diseases and the reform of home care services. The second finding is a wide variation in the positioning of all 47 ESAs studied, regardless of the region examined.
This quantitative analysis was supplemented by a qualitative analysis conducted among ESA professionals. We analyzed the three groups of ESAs from four perspectives: 1) the characteristics of their service area, 2) the presence or absence of caregivers, 3) the MMSE scores of the clients they serve, and 4) the size and profile of their staff.
| Group 1: Complies with ESA specifications | Group 2: Significant deviation from specifications -20% (FTE and/or active cases) | Group 3: Furthest from the specifications (FTE/Active file) |
|---|---|---|
| Geographic Area: 29% of home care agencies travel more than 30 km to reach their clients’ homes Caregivers: Group consisting primarily of clients accompanied by a caregiver Clients: Significant proportion of clients with severe MMSE scores Staff: Full HR team |
Territory: Group traveling the fewest kilometers to reach its clients’ homes Caregivers: Group with the highest number of clients who have caregivers Clients: Care for clients with more complex needs than Group 3 Team: Group with fewer ESA staff members and a shortage of ASG and occupational therapists/psychomotor therapists. When this is the case, the ESA staff reorganize themselves more effectively internally to compensate for the staffing shortfall |
Territory: Group traveling the greatest distance to reach its clients’ homes Caregivers: Group with the lowest number of clients who have caregivers Clients: Cares for fewer elderly and severely disabled clients than Groups 1 and 2 Staff: Group with the most FTE ASGs and understaffed occupational therapists/psychomotor therapists, as well as organizational difficulties. It is the only study group with FTE IDECs exceeding the number specified in the specifications |
Note: There is no significant difference in the particularly long wait times for patient care among the three groups.
Analysis: The challenges associated with travel distances and the care of patients with severe cognitive impairment (MMSE score below 10), the very elderly (over 90 years old), or those without a caregiver appear to be surmountable if teams are reinforced internally (including with psychologists, occupational therapists, or geriatric care assistants (ASG)). Care is then reorganized: occupational therapists take on the tasks usually assigned to coordinating nurses (IDEC) and manage the first and last sessions. ASGs focus on the other care sessions and can also provide support for the ESA’s administrative tasks (in collaboration with occupational therapists/psychomotor therapists).
On the other hand, if the shortage of full-time equivalent (FTE) nursing assistants and occupational therapists (or psychomotor therapists) is not addressed, nursing assistants face three challenges: caring for difficult patients, traveling long distances, and maintaining a caseload that meets the requirements of their job description.
C. RECOMMENDATIONS
The practices of professionals at the 40 ESAs in the Grand Est region vary from one ESA to another depending on the context, the profiles of the users, and the working conditions. This diversity also presents an opportunity for professionals to engage in a collective discussion on best organizational and managerial practices across several areas:
For users:
In terms of targeting and prioritizing users:
- Target users based on their level of cognitive decline (MMSE score, etc.) and establish prioritization guidelines to standardize practices:
- Provide care for users with an MMSE score of 15 or higher in accordance with the ESA specifications:
- Involve the caregiver - Organize routes by sector using the SSIAD transport units to optimize the area covered.
Regarding the delivery of sessions:
- Limit the number of sessions to what is necessary to achieve the goals (fewer than 15 if the goals are met sooner) and do not exceed the maximum of 15 sessions.
- Coordinate the professionals involved in the initial sessions.
- Tailor the content of the sessions to users' needs (cognitive stimulation vs. rehabilitation).
In terms of mobilization as well as support for caregivers:
- Involve the caregiver more in the care process.
- Standardize assessment tools for caregivers at the beginning and end of care (e.g., the ZARIT scale).
For the organization:
In terms of organizational structure and human resources training:
- Pool ASG positions with the SSIAD, as well as psychologist and administrative staff positions, through integrated structures. This pooling of positions makes it possible to offer full-time positions to professionals (between the ESA and the SSIAD) and to enhance the program’s appeal
- Set up an automatic replacement system for extended leave or absences (similar to the replacement pool used in nursing homes, with staff from the parent organization sharing the workload).
- Revise the terms of reference for the ESAs regarding human resources (positions and FTEs)
- Offer the COTID training program to all ESA professionals[6].
To improve the experience:
In terms of the ESA’s presence in their local communities and with their partners[7]:
- Standardize tools and methods among the various care providers in the region to reduce late referrals or referrals of patients with an MMSE score that is too low
- Improve coordination with private practitioners to reduce fragmented care, which can sometimes lead to gaps in the continuity of care
- Strengthen and facilitate access to transitional care facilities in certain areas (fee-based facilities located far from the patient’s home, alternating between group care at day centers and care at the patient’s home, which can sometimes leave certain patients more vulnerable)
Furthermore, ESAs would benefit from improving communication and strengthening coordination among themselves as well as with their partners, particularly independent practitioners, referral agencies, and coordination support units (DACs). The use of a secure, shared platform across the region would streamline the transfer of medical records when a user is taken into care. This tool would also facilitate communication among ESAs (exchange of best practices, user transfers, etc.) and contribute to smoother user pathways. An organizational structure for ESAs that clearly defines the sharing of roles, responsibilities, and care protocols with DACs would enable more effective user referral.
Conclusion
This overview of the ESAs in the Grand Est region provides insights into three main areas: the ESAs’ area of operation, the organization of the ESAs—including caregivers and their partners—and the ESAs’ compliance with their terms of reference.
ESAs are required to cover the entire territory of a region; however, when faced with constraints that sometimes lie outside their scope of responsibility, they adapt using the resources at their disposal to meet users’ needs. However, it is important to note that certain underserved areas face structural barriers (lack of prescribers and/or supporting infrastructure in certain territories) but also have factors that facilitate the implementation or deployment of new ESAs (available staff, effective coordination with partners). It is sometimes necessary to redefine the service areas of ESAs to limit overlapping service areas.
75% of the ESA agencies evaluated in the Grand Est region regarding the FTE/active caseload criteria fall short of the specifications. Since these specifications date back to 2012 and user needs have evolved, it seems appropriate to adjust them in terms of missions, staffing levels, and funding, even though harmonizing practices across ESA agencies could lead to greater compliance with the specifications. In fact, practices can vary significantly from one ESA to another, whether regarding user selection, route planning, caregiver supervision, or the organization and content of sessions. A key factor in the success of ESA operations is the pooling of team professionals with those of the SSIAD, particularly to enhance the appeal of these professions.
Priority should be given to ESAs that have established partnerships, particularly with teams from the Coordination Support Units (DAC) and private practitioners, as these stakeholders are essential to ensuring the relevance of the care pathway and the proper referral of users. For ESAs, this involves sharing information about their internal structures, their methods of intervention, and the roles and responsibilities of each team member to ensure that user referrals are as appropriate as possible.
Notes
- The reform of home care services and the future national strategy for neurodegenerative diseases will affect how these facilities are organized in relation to one another, including their affiliation ↑
- https://www.agevillage.com/outils-et-fiches-pratiques/7642-1-mesurer-la-qualite-de-vie-des-personnes-atteintes-de-la-maladie-d-alzheimer ↑
- https://www.hug.ch/sites/interhug/files/structures/soins_palliatifs_professionnels/documents/grillede_zarit.pdf ↑
- The ESA specifications date back to 2012. Under the leadership of the Directorate General for Social Cohesion, work is currently underway to update the ESA specifications. For ESAs authorized to serve 10 or fewer clients, their active caseload and FTE figures have been reported based on 10 clients to facilitate comparison. ↑
- Groups 1A and 1B comply with the specifications; however, Group 1B differs in that the ESAs in this group have administrative staff or psychologists assigned to them, which is not provided for in the specifications ↑
- The COTID training program is now more widely offered to occupational therapists and psychomotor therapists. ↑
- Internal coordination within the ESA team is necessary to ensure optimal care before collaborating with the DACs. Furthermore, strengthening ↑

